Chapters
Show Highlights
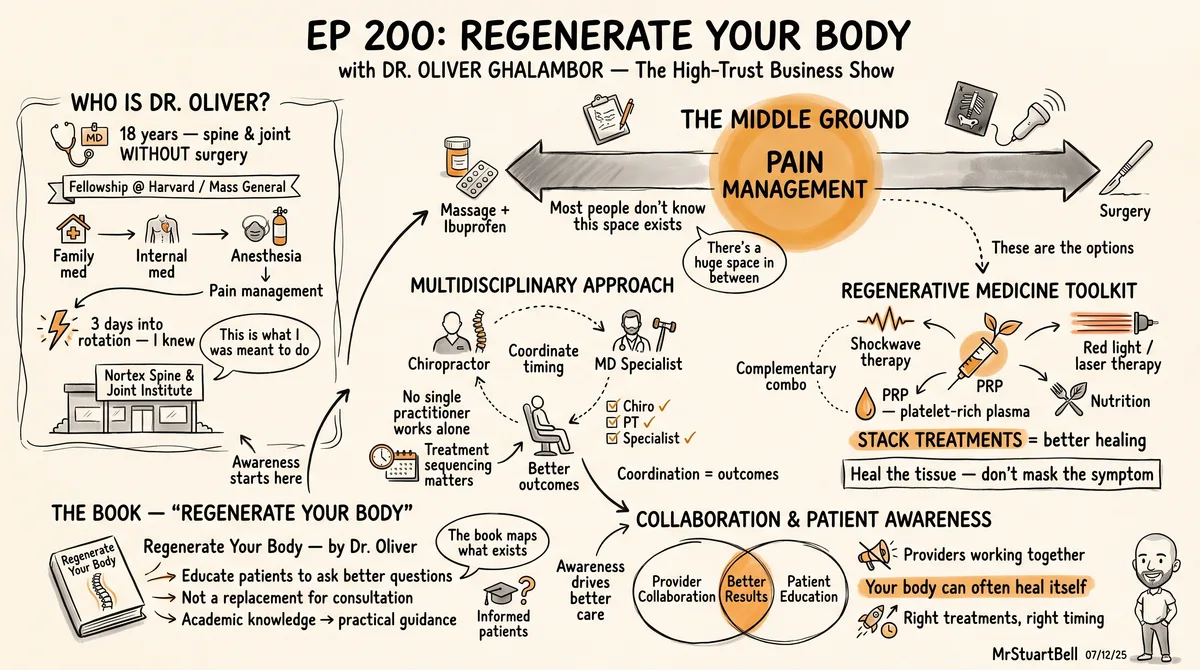
- Pain management isn't just pills - there's a whole spectrum of interventional treatments between massage and surgery.
- Multidisciplinary care works best when chiropractors, physical therapists, and medical specialists coordinate treatment timing.
- PRP therapy and other regenerative treatments focus on healing underlying tissue damage, not just reducing symptoms.
- Stacking complementary treatments like shockwave and red light therapy creates better long-term recovery outcomes.
- Your book should educate patients to ask better questions, not replace professional medical consultation.
- Collaboration between healthcare providers delivers better results than any single practitioner working alone.
There's a huge gap between popping ibuprofen and going under the knife for spine and joint problems. Most people don't know what exists in between. I talked with Dr. Oliver Ghalambor, who's spent 18 years treating patients at Nortex Spine and Joint Institute without surgery. His new book "Regenerate Your Body" maps out treatments that actually heal underlying issues, not just mask symptoms. Oliver discovered interventional spine care during a residency rotation and knew immediately he'd found his calling. His clinic uses a multidisciplinary approach combining treatments like PRP therapy, shockwave, laser therapy, and nutrition to help patients avoid the operating room. We talked about how regenerative medicine has evolved and why patient awareness matters. Your body can often heal itself when you stack the right evidence-based treatments together. Oliver breaks down how to move from academic medical knowledge to practical guidance that helps people ask better questions about their care.
Transcript
AI transcript provided as supporting material and may contain errors.
"Awareness from pain management kind of being more than just pain pills and being more a place between less invasive treatments. You know, there's between chiropractic care, massage and ibuprofen and getting caught on. There's a huge space and that space is called pain management."
Stuart: Hey, welcome back. Another episode of the book More Show. It's Stuart Bell here and Today joined by Dr. Oliver Gaur. Dr. Oliver, how you doing?
Oliver Ghalambor: Good, good, how are you?
Stuart: Yeah, very good, thank you. It's always great to have conversations with people who we've written books for, particularly when I'm been involved so much in the process that obviously we've been doing this for a while, knows it usually moves through pretty smoothly. But I like it because I've had chance to see the, the books, how the process come together and what the external view is of what you do. And then in these conversations it's good to put some meat on the bone and talk a little bit more. Really almost like the clients would have that same exposure. They kind of see you through the book and then see you in real life. So I always enjoy these conversations. Why don't we start with a little intro on you tell the share with the listeners what it is that you do and then we can jump off from there.
Oliver Ghalambor: Yeah. So I'm a physician, I'm md and after a rather long path, I did family medicine, internal medicine, anesthesia, but I ended up doing my fellowship in what is called pain management. But in all reality is interventional spine and joint at Harvard Medical School, Massachusetts General Hospital. And since I graduated almost 18 years ago, this is 100% what I've been focusing on, treating patients with spine and joint problems with non surgical interventions. So that's, that's me in a nutshell.
Stuart: That idea of going into spinal joint straight out of school. Did you go to school expecting that to be the path or was that kind of the path that you took when you were going through the training?
Oliver Ghalambor: No. So, you know, obviously in the beginning I had bunch of thoughts. At some point I wanted to become a gynecologist, cardiologist, surgeon, whatnot. But eventually I was doing my residency in anesthesiology and I loved it. You know, I would have been a happy anesthesiologist, not as happy as right now. But so as I was doing the residence, the residency in anesthesiology, we have a couple of rotations. You know, we have rotations in icu, we have rotation and you know, obgyn, anesthesia and putting epidurals and whatnot. But one rotation was in the pain management department. So I got exposed to doing X ray guided. Basically at that point, ultrasound was not a thing yet, mainly X ray guided interventions on the spine and joint. And after three or four days into that program was like, yes, this is what I was meant to do. And so, you know, by the end of that one month rotation and pain management, I pretty much was decided that's where I want to go and apply for fellowships.
Stuart: Yeah, that's fantastic. I'm always having to had a career that's jumped around a little bit over. You can tell by the gray in my beard that I've had long enough time to go through a couple of iterations. But it's always interesting to see people who really find their passion and know what it is pretty early on because you've got such a opportunity to really double down and specialize that approach of pain management. With the patients that you see now, are they coming in typically looking to avoid a surgical intervention or are they just coming in with symptoms and they're not necessarily, they don't know what the fix is, they're just happy to have the problem resolved?
Oliver Ghalambor: Well, kind of both. Right. And so, you know, the challenge that we have is that there are multiple people, including providers or non providers, that you can seek help when you have a spinal joint problem. Right. You know, you can, you can just go get a massage. If it's not that bad. You can pop in over the counter ibuprofen, tylenol and whatnot, go on online and buy a device that looks like a tens unit from Amazon and then inversion table and you know, try to mimic what some other clinics are doing, the true decompression of the spine. So yeah, so we have, we have a bunch of people looking at bunch of angles. And one of the problems is that this is what we call a fracture type of a care. You know, so when you go to your chiropractor for your back, most of the time they almost exclusively want to treat that problem with chiropractic care. Now chiropractic care has its place and it's not just one treatment. They also have a gamut of multiple, multiple treatments that they can offer for say, somebody with back pain. But you know, a cooperation between providers, hey, this is, I think this is the one that needs to hand in hand be treated with the interventional spine and joint specialist is what we call pain management still. And at the same time, you need to do physical therapy at the same time. So basically what we call a multidisciplinary approach when a team is there, or at least even if you're not under the same umbrella, to be aware of what other people do and be open to work with other colleagues is the ideal situation. So that's what we have. So a lot of my patients initially don't come to see pain management or two for treatments. They come see initially to see our chiropractors. They're like, well, hey, I have, you know, arthritis of the knee, for example, and it's bone on bone. Well, that is one of the situation really. Okay. You know, some help could be achieved from chiropractic care. Some help could be achieved from physical therapy strengthening the muscles around the joint. But really, you know that that pathology needs to be treated by an MD interventional spine and joint specialist early on. Now, once the symptoms are better, then yes, that's the time to strengthen the muscles around the knee that have been, you know, had disused atrophy. Right. They're, they become lazier and that creates another problem if you don't fix it. But when people are miserable, you know, seeing a chiropractor or a physical therapist is, you know, you really don't get a whole lot of return on your investment, basically. But just, you know, a short answer of that would be people typically come for symptoms and then from there, depending on where they end up, if they end up in the primary care office or at orthosurgeon office or chiro office, they may or may not cross paths with interventional spine and joint specialists. And that's one of the main reasons I wrote this book is to kind of describe not only what our specialty is, but what our specialty can offer today in 2025.
Stuart: Right. That specialty has that developed. The rate of change of that development has that really accelerated over the last few years. So it's maybe a situation where even people who are in the, in the industry or that they should be in the know maybe don't know the full extent of what the options are. Kind of like that fast moving, it's difficult for people who aren't very narrowly focused on to really keep even if they're, they're broadly in the medical sphere. Or is it that it's really, it's stayed the same for a period of time. It's just that people aren't necessarily aware of it. What's the big driver for the kind of the knowledge gap? Is it just a general lack of understanding or is it just like a speed of changing? Hey, this is really what we could do today.
Oliver Ghalambor: Yeah, I Mean, it is both. So you know, as far as awareness, unfortunately like 10 years ago, 20 years ago, the family doctors only would send people to pain management only if they asked for narcotics. Not really helping, hoping they would get any triplets treatment. And they thought, well, the real fix is eventually to get a surgery and fix, quote, unquote, fix the problem. But uni, unfortunately a lot of people have learned the hard way that you know, a surgery is not really fixing the problem. If you had your, you know, God given knee joint or spine, if you had the original parts and that's, that's, you know, I have more problem with guys. I don't know why, especially if they're, if they're like driving a Harley or whatever. They kind of think of a body as a motorcycle or a car or whatever. It's like, well, if it's broken, then let's fix it. You know, it's like, well, yeah, I mean if we had, you know, another tire that was identical to the one you had before and we could replace it, sure, you know, go ahead with it. But we just don't. What we do, what I tell people is, you know, imagine you're replacing a rubber tire with a metal tire or even worse, a metal tire that is square.
Stuart: That's actually a funny analogy.
Oliver Ghalambor: Like do you want us to work with a tire that is not fully inflated or do you want to go get his metal square tire? And that's where like oh, oh, okay, well, you know what, never mind.
Stuart: That's actually such a great analogy, isn't it? Trying to bridge it into something that's more accessible and we can see and it's more tangible sometimes kind of things that are underneath the skin. It's kind of outsider of mind. You just imagine like a hot swap, pull one out and put one in to not exactly being a like for like it really to you to think about. Okay, well is that the best option or is there something a little bit more sensible to do?
Oliver Ghalambor: Right. So yeah, you know, awareness from pain management kind of being more than just pain pills and being more a place between less invasive treatments. You know, there's between chiropractic care, massage and ibuprofen and getting caught on. There's a huge space and that space is called pain management or interventional spine and joint. And to your point, the field has been evolving and to a scary actually speed right now to the point that even, you know, I've been in this space and it's what I do every day and anytime somebody brings up something I Read about it because, you know, I. I'm a lifetime student. All doctors should be. You know, that's what I signed up for. But still, when I was starting to, you know, write the book, you know, I wanted to just get on top of what is there right now. And I was like, wow, you know, there's so much stuff that I learned, right, Being pushed to write a book.
Stuart: And that is such an interesting point because it's sometimes, particularly when we're in it every day and we think that we're in a engaged way, so we try and keep up with things. Unless there is an external force, like writing something in a book without that external source of actually diving in a little bit deeper and thinking about the latest or questioning new assumptions or writing so much and wanting to check something and then finding that next level of detail that has come up more recently. Such a fascinating opportunity because you wouldn't necessarily. Once we've left school and aren't forced to write papers on things, you don't necessarily have the luxury of taking that time to actually sit down and go through that little bit deeper. Even, as you say, being the expert and in it every day, it's about how fast things move from the patient's perspective. Do most people come from referrals from other practitioners or most people doing their own research and then getting to you from their own kind of own desire to find something?
Oliver Ghalambor: Yeah, so most people come from referrals. And again, like you mentioned, with symptoms, hey, I have knee pain. You know, what can you do for it? But interestingly, more and more people have been in the last couple of years coming and asking for specific treatments. And these are the regenerative medicine treatments. Prp. Hey, do you guys do prp? And every time I get that call makes me so happy because finally people are just trying to, you know, they're learning, they're learning that there's more. And that's that, that the, the regenerative medicine, and that's what the book is about, is been a game changer has been a game changer in the last couple of years. And that's what I've seen. You know, in the, in the beginning when I got trained and started practicing, we did not have it. We did not have it. Then we started to, you know, do some of it. And then good publication came out. Early pathologies, there were tennis elbow that were being treated with PRP. And they, they, they showed there's more than 90% of people get complete resolution of these symptoms last. And that's something we're not used to, we were not used to, we were used to. Well, hey, we're going to get a cortisone shot and more likely than not, you know, that would just get the inflammation down. Symptoms are better, but the tissue actually doesn't heal on its own. And then six months, a year or two later, they will be back, you know, so they, they used to call these pain clinics Hotel California. Right. You can check out anytime, but you can never leave here. Yeah, but the results of medicine has been a game changer because what we're doing here is that a lot of these structures that don't heal is because they don't have any vascular apply. So not a whole lot of repair material that are readily available in the blood can make it to the, let's say the cartilage or the meniscus of the knee or the tensile tendons of the tennis elbow. And so the body cannot just fix it. You know, it's not like a skin or muscle. You cut it, in two weeks, you're all healed up. These structures that don't have vessels can't. And so the idea of, you know, our early on present of medicine, treatment, which is the PRP platelet rich plasma, is to get what we have readily available in the blood or in you know, severe cases, the bone marrow ourselves, isolate them, concentrate them and put them exactly where they're needed. And that would start a healing process. And so that's, now we're no longer talking about just getting the inflammation down and getting, treating the symptoms, were actually treating the pathology, pushing the body to do the repair and fix it.
Stuart: Yeah, it's so interesting is that, I mean there's the upside and the downside of Internet research. I mean there's that meme of I've, I've got, my nose is dripping on, my head's aching and within two Google searches it's some kind of tumor, cancer or something catastrophically bad. Just the nature of the beast. But the reality is that people I think these days are a little bit more savvy at doing some research and the availability of information and people's ability to decipher a little bit, it's not just superficial. They can go down and get that level of information. It really is meaningful. So it's always interesting when we're bridging that gap from a knowledgeable audience where there's the beginnings of some kind of, they know kind of what they're looking for, but they don't, don't know the specifics. I Think a book is such a great opportunity to kind of bridge that gap for them because it's a easy way for people to identify as yes, this is what I'm looking for. It's a low commitment way of. It's not like they have to come in for a consultation. It's an easy way to start that conversation. But it really steps them through in a slightly more meaningful way than just a two minute video, slightly more meaningful way into whatever that next step is. So when the book itself is called regenerate your body and heal, which is such a perfect title for exactly, exactly what it does on what it says on the tin, do you find people are looking for those kinds of regenerative based answers? Kind of coming from a place of kind of knowing what they're looking for, but not quite. Or as you were saying with the patients who were coming to the clinic previously, they're really looking for resolution to a pain situation. Do you find most people are aware of regenerative medicine as an idea or is it really they're looking to fix penis, elbow or a problem with the spine?
Oliver Ghalambor: Yeah, so most people at this point in time are aware of regenerative medicine. I think PRP is becoming more and more something people are more familiar with. But almost everybody knows about quote unquote stem cell injections. And you know that that is also a topic that I wrote my book. The challenge is, you know, yes, people became aware of their options but then there was a lot of false promises and bad players in the space. The FDA not allowing any lab to get basically certified in the US and flat out saying, hey, we don't want anything live from somebody be injected into somebody else. You know, pushed some of these, you know, companies and scientists out of the country, the ones that were doing it here, they were promising something but then they couldn't because their hands were tied up. And so we have some people that have paid a lot of money in the US and or have gone abroad without really getting any response. And so people are kind of aware of the stem cell prp, regent of medicine, but they're also kind of at this point suspicious. And the edge, they, it's not like when it came out and you said you threw that name and they will just go for it and now they, they want more. And like you said, the Internet is amazing. You know, it is a double edged sword. Right. In my opinion, if you use it the right way, it is really good and I always encourage doing it. And by the right way, I mean if you just Go and say low back pain, what to do. Right. So that's not a right research. Then you know, what you're going to be hit on with is the paid advertisements that will come up. They wanted to sell you stuff and whoever locally has the biggest budget, you know, be at the hospital chain or whatever pushing their, you know, trying to get their ORs busy with surgery, you know, will pop up and whatnot.
Stuart: So that's.
Oliver Ghalambor: But you know, once you either get in front of a colleague of mine or myself, talk about the. Okay, this is what we're going to do. You know, this is specific part of your spine, let's say the facet joint. The joints of your spine have arthritis and the plan is to put PRP in it. So you can either, you know, learn that by, you know, consulting a colleague or you know, again, this is a book, you know, and the book is symptom based as well. So you know, if you have back pain, what protocols we have in 2025. And of course it goes into whether it's from the disc or from the joints. But let's say we have identified that the joints are the problem. If you then put research affiliated with facet problems of the spine and prp, you would get beautiful data to the point that, you know, if you spend a couple of hours of it, you probably would be more knowledgeable about the research out there than I am. It's impossible for me to retake or any doctor to retain all this information that is out there. There's plenty. So if you narrow and know what you're looking for and narrow it down to your pathology and the treatment that you're going to, you know, take it is. It is, it is wonderful. It is wonderful.
Stuart: I think that point of people being a little bit more specific and really dialing in on the details is. I was doing some work this morning with ChatGPT and similar kind of as we were talking, we were talking about the, the acceleration over the last even six months, 12 months of that world. But also the specificity, like asking for something relatively high level and generic, you're going to get a response. But really once you start drilling down and as your knowledge increases and the quality of the questions you ask also increases, the questions of the responses come back. And I think that's what I really like about the approach you took in the book. Not only is it a kind of high level overview of the subject for people who have really no knowledge, it also then gets very specific on the individual symptoms and pathologies, as you mentioned. It gives people the opportunity to see themselves a little bit more in the details and recognize what the next steps are. So when they do take that next step and reach out to you, the conversation is just so much more elevated than it is if they just walked in off the street. Was that intentional in the fact that sometimes you have conversations they have to be very, I don't want to say superficial, but very high level. And I know that people really, really do want to drill down into the details, the structure of the book. Is that a reflection of the experiences you've had?
Oliver Ghalambor: Yeah, certainly. You know, I, this is like I said, five days a week for the last 17 years. I see what people most number one or two or three most common problems are and then how we have been able to combine the treatments that we have right now to address them. And you know, I, you know, it's like, well, you know, this is what I'm doing, you know, to help my own patients to understand. Let me start with a book. And as I started it, you know, again, I wanted to make sure I'm on top of everything before I think. And I probably bought 60, 70 books on Amazon. Now, of course I have my own medical books. What I'm talking about are the books that are for general population, for the patients, non physicians. And so I bought about 50 or 60 books from Amazon. And, and yeah, they're great books, let's say of any treatment modality per se. There's phenomenal book just for prp. They're books about stem cells that really dig down deep into the details. There's book about nutrition, there's a book about laser therapy, red light therapy, all these treatments, exosomes, all these treatments that I mention in the book. There is one specific book for that treatment modality out there that is way more detailed. But I never got a chance to find any book that says, well, if you have Tennis elbow in 2025, these are the combination of non surgical interventions that you can combine. When we talk about combining treatments, we call it stacking. Stacking treatments. So let's say you use the prp, but also you use a shockwave and then you also use laser on it. And also you take supplements and also you inject peptides. So these are all treatments that just synergistically help each other. So stacking. So what is. And you know, again, if you search online, you might have a lot. If you go to gnc, they want you to take the entire store as a supplement. But what are the top, let's say 6 to 10 proven evidence based treatment modalities that you can stack and maximize the relief and the regeneration to hopefully once and for all heal and stay away from invasive therapy. That's what the book is all about.
Stuart: And such a great approach because so often we really do. People hear me talk about it all the time. This separation between a traditional book where the job of work, the purpose is to sell the book and the whole thing is about the book, and a conversation starting book where the purpose is to help someone show them the next step. But then the next step is clearly out of the book and the book itself isn't really the thing the conversation is being and the approach that you've taken of understanding what those conversations are and then just replicate them in a book format that makes it accessible and easy and gives someone, gives a real person a real understanding of the real problems that they're facing, the real next step they can take. I think it's too easy for us, especially if we come from. Well, I couldn't say we could. I really don't. I can say, well, if we come from academic background, so we get into this traditional academic way of thinking about writing something that is then peer reviewed and marked and, and scored and redlined, all of these kind of traditional ways of writing that were taught from kids. It kind of does a disservice for the rest of us who don't resonate with that and find that difficult to do. The reality is the knowledge is in our head. Even if we have to go and get some books just to make sure that we want to be as up to date as possible, the knowledge is in our heads. And if someone walks through the door, we know the conversation is really meaningful for them. And if we can capture that in the pages, then it's done its job because it really is helping people take that next step. Coming from that academic background, did you find it difficult making that separation between something that this isn't a peer reviewed because it gets on PubMed or whatever this is. This is something slightly more informal, very valuable, even more valuable in a sense, but informal. Did you have a problem making that kind of psychological switch between the two?
Oliver Ghalambor: Yeah, definitely. I think any MD that is working in the musculoskeletal space should, you know, open their mind and you know, as when we go through academia, if you will, and any treatment that has not had a randomized double blind control study cohort follow up of, I don't know, let's say 10 years plus is basically refuted. That is an approach 100% academic person, which has its place. The challenge is there are a lot of times where it's not possible or it's not ethically possible or physically possible to make people with some pathologies to one group, we're really not treating it. They're the control subject and the other.
Stuart: Right.
Oliver Ghalambor: And so we have to open up our mind. I mean, I was doing it already. I was, you know, going to Harvard and doing my fellowship in spine and joint, but simultaneously I was going to the Harvard acupuncture class taking courses because it was. It was awesome. And so that is the exact opposite. There is no random control studies on anything acupuncture. In fact, you still don't know what, you know, the mechanism of action is. You know, they say how to do it and. But, you know, so that's a complete opposite. That's a kind of a trust me, bro, type of science.
Stuart: And at least if people are going in with their eyes wide open, I mean, at least it's. If everyone's transparent about it. But it is interesting. The real, like you were saying before, the difference between a massage and being a surgical intervention, there's a lot in between. I imagine that's the same at Harvard. You've got classes that are one in the spectrum and then at the other.
Oliver Ghalambor: Right. And you know, the same thing. You know, once, once we want to work with our colleague, physical therapy, chiropractic, massage therapists and whatnot. They don't have the same type of, you know, strict mindset. And, and it is, it is musculoskeletal. And it's. That's. That's how it is. We don't have. It's not like infectious disease. You know, you have an infection, you. You culture, you find the, the bug and then, you know, they're exactly sensitive to antibiotics. Abc. And not susceptible to others, you know, Exactly. Antibiotic A, this is this many milligram per kilogram once a day for 10 days. That's standardized across the board. Everybody agrees to it. That, you know, we have specialties that are like that. When, you know, let's say cardiology, you have chest pain, you go, there you go. Cardiac Cath. It's above 90%. You can standardize this. When it comes to having, you know, let's say disc herniation and sciaticon back pain, there are some, you know, so there are, There are definitely indications. If we have weakness anomalous in the leg of somebody with a new disc herniation, we do want to immediately send them to a Surgeon. And so consider the skip. And so we do have some guidelines that are black and white and these are typically for, you know, urgent or emergency cases. But you know, you've had back pain on and off for 10 years still. The reality is, you know, you go to multiple providers, even if they've been trained the same way, depending on thought process and their own personal experience and their knowledge base, you could have different recommendations. So definitely with muscular skeleton you have to keep an open mind.
Stuart: Yeah. And again, that's what's nice about the book because it does give that breadth of understanding as someone's looking through it. They can narrow in first on the symptoms, what they believe are their symptoms or the outcome, the intervention that they're looking for. But then there's other information that's broader that helps widen that conversation. And it, the, I think it really is the case that books have a way, even if people just look at the table of contents to a certain degree, it's still structured in a way that helps expand that thinking and gives more meaningful questions to answer. Next, whether they read 10 pages of it or 100 pages of it, the idea of the book and getting that in front of people so the usage of it, did you have a plan when the idea came to write it and then bringing it together, did you have a plan of sharing that more with other people, practitioners and professionals, or direct to consumer or existing patients? What was the thinking around how it was getting out in the world? Do you have any particular band?
Oliver Ghalambor: I mean, definitely it's a patient level book. My colleagues are certainly aware of all these, you know, treatments, or they should be. The challenge is even though they're aware of it, they don't necessarily recommend it. So you know, you end up at a, at a surgery clinic and the ortho. Fortunately, a lot of orthos have embraced PRP treatments either before or in conjunction with their treatments. For example, we know that if somebody has rotator cuff tear and they need rotator cuff surgery, injecting PRP right after the surgery in the OR would actually accelerate the healing process, decrease the post pain and decrease the chance of re tear. So sometimes you, you, you fix the rotator cuff, but it tears again despite the surgery. And so a lot of authors are aware of it, but that's kind of the extent of it, you know, and then maybe they will recommend physical, I mean for sure, definitely they would recommend physical therapy. But a lot of those just this just, they just fail to say, hey, you know, by the way, this is what you have to take. For your body to have the building blocks, you have to have enough amino acids, you have to have these supplements. And these are the studies that show that if you do these, your post op healing is accelerated. So the nutrition part, you know, we just don't, you know, a lot of orthopedics, hey, I'm, I did the best surgery possible or you know, same thing, you know, shockwave therapy, red light therapy, class four laser. These are the treatments that are there. Everybody's aware of them, but they don't necessarily top of mind and it's like if you have and they don't, you know, they, it just, maybe they're too busy. It doesn't. But a lot of times what I want patients to do is to ask a provider, is there anything else that could help me in addition to the surgery, for the surgery to be successful or to avoid surgery and that typically my colleagues, yeah, okay, yeah. By the way, you can do abcd. But yeah, so I guess the purpose of the book was number one, increasing awareness of the patients themselves. And then number two, you know, just a reminder to my colleagues, hey, you know, these patients, don't forget that these are also the options that can help your, the treatments that you're doing. You know. So to my colleague, colleague, chiropractor, hey, if you're treating, you know, you could also, if you're not getting the result you want, these are other options that
Stuart: you can such a great opportunity because this idea that again listeners to the show will have heard me talk about before, this idea of complementary non competing businesses, all of these other practitioners fit in that, that mold and positioning the book as a tool that makes their work more, more, I don't say more successful but it enhances the overall patient experience and highlights their work. Instead of it being a directory placement, it's an enhancement to it. And a book is a way of kind of communicating that message in quite a non threatening way. It's not like you're going in there and saying, oh, you need to tell them to do this because otherwise your work will be unsuccessful. It's hey, you did a great job of what you did. Now here's an opportunity to share with them some other things that might be beneficial as well. So that not complimentary, non competing opportunity to raise the whole tide is.
Oliver Ghalambor: No, I mean that was not, not presses them towards any specialty. And I, you know I mentioned chiropractors and in fact chiropractors were one of the early adopters of the shockwave therapy and the laser therapy way before the pain management and the orthopods did it. So, so they, they. Their mission is pretty much the same as us. Try to do the least invasive treatments first and combine as many treatments together as you can. In fact, and been working very closely with a colleague of mine, Dr. Wojnicki, here in town. I'm located in Allen, Texas, close to Dallas at this point, after we talked and we're now actually writing a book together, which is the Chiropractic Care and Regenerative Medicine. How that fits into each other. Because like I said, the vast majority of patients that don't want to get surgical interventions with spine and joint problems end up at the chiropractor office first. They bring it up to their family doctor was like, no, no, no, no, no. If you say your family doctor, you have back pain, next thing you know, you're sitting in front of spine surgeon talking about surgery. You choose between surgery A, B or C.
Stuart: Yeah, you've got all the choice in the world, but it's AB or. And Sanjay, it's quite an interesting point as well, isn't it? Because as no matter what industry you are in, there's certain zeitgeist or narratives out there in the world that the patients have got, rightly or wrongly. But it's interesting to be aware of those and then try and intersect with some of them as well. So rather than trying to fight against the tide, kind of understand what's going on out there and then intersect in the conversation a way that you can make. It's still early enough to have a meaningful, meaningful difference. And to your point, the whole idea of a holistic approach to health care, it's not just one provider doing one thing at the exclusion of everything else. More and more evidence and more and more examples of people having much better outcomes in that way.
Oliver Ghalambor: And one thing I wanted to mention is that, yes, you know, we're really focused on musculoskeletal, spine and joint. But I did in the book touch on the entire body as well, if the entire body is functioning as a unit better than any part of your body that needs healing. And so that comes into longevity. Right. And so right now, it's a hot topic, you know, and again, same thing. There's a lot of information out there and sometimes a little hard to even kind of decipher what is real, what is not real and whatnot. And God forbid, you know, you type that in Google in five minutes, Facebook and Instagram will choose to ask for supplements.
Stuart: Yeah, yeah, yeah.
Oliver Ghalambor: They are related. They are related. It, you know, one of the, you know, whoever wants to live longer and happier, you know. So we were talking about longevity as far as like the lifespan, how many years you have. But also we're talking about the health span, how many of the healthy years you have. Right. And so a lot of people agree that yeah really health span is where it's at better than lifespan. And both of them, the number one non, non medical, basically the treatment, the one that you don't take a medication on your own, the most powerful treatment is. Is exercise for both increasing your health span and lifespan. And then, but yeah, if you have a spinal joint problem that then will deny you access to that drug. And so that's where my field comes in. But, but the ultimate goal is not to fix your knee and then you just, just sit and watch TV and do nothing with it, you know.
Stuart: And that's a great point on the recovery and the holistic approach with the other disciplines as well as you kind of transition out of one stage into another stage that that starting discipline isn't necessarily going to be fit for the next stage because just the physicality and your health moves into a different place. So treating the body as a whole and health span over lifespan and the quality. It's such an interesting time where we are now because I think there is the. Well, again it might be your point that when you as soon as you google one thing everything is. You get inundated with the same thing. So it might be. I'm interested in this space health span generally. So I naturally tend towards some of that content, which means I get shown more content. What I was going to say was we do seem to be on a bit of a cusp and a turn where for the last 40 years or so maybe there was not really that much attention paid to healthspan because everyone was generally healthy anyway to a certain degree and lifestyle choices were different back then, which didn't have such a dramatic impact. Then there was not really paying attention to it. But everything kind of changed a little bit. So things got worse. Then there was a kind of a. Hopefully a drug panacea of well I can do whatever and there'll just be a drug to fix it. Now at least we do seem to be changing into it, people being more aware and, and taking some accountability. So hopefully over this holistic approach to healthspan is going to be something that becomes more and more prescient and on more and more people's minds going into the future. Which again comes back to the book is a great tool of helping start that conversation. And whether it's with people themselves searching for it or other practitioners who could refer it or existing clients, obviously they're hearing conversations out and about in the world. And as we hear about our should get a copy of. Let me get you a copy of Dr. G's book because this is the information that you need. So yeah, such a fantastic way of bringing it together. Everyone who's listened to the podcast will hear me get to this point in the call and look up at the clock on the screen and realize that time's gone by. It goes so fast, these podcasts. It's really fun talking to people, particularly when they've got a passion about their subjects, because it comes through. Before we wrap though, I want to make sure that people can find out more about you and what you do. So where's a good place for people to go to find out more about the about you in the practice?
Oliver Ghalambor: So my practice is called Nortex N O R T X basically abbreviated for North Texas Spine and Joint Institute. And so the website is up. We have now a section of the department that is geared more towards helping to tissue regeneration. Right. With combining stacking, treatment modalities, PRP, red light therapy, laser shockwave therapy and SO3 that is called Nortex Tissue Regeneration. And we're, you know, on web we have the website, we have Instagram and Facebook and basically the social media.
Stuart: Perfect. Well, I'll put a link in the show notes to those resources so as people are listening or on the website on podcast players, they can just click straight through. And again, it's a subject that I'm pretty passionate about for myself and our family kind of that, as you say, lifespan isn't really anything with, with that health span. My dad, it was my dad's birthday a couple of days ago and he's in his mid-60s and is still up and about and, and remember a story. I'm obviously over in the US now and they're back in the uk. So I called them last year sometime and my dad was talking about gardening as it was going back this time of year going into the spring, and he'd been gardening in the. The trash cans, the wheelie trash cans, the gardeners. The yard is slightly raised, so he was piling the trash cans up and as he was getting full of guard yard debris, he stepped in it to push it down a little bit and at 85 years old kind of stepped in and then overbalanced completely because as he stepped on it, it just disappeared and then he rolled over and did a forward roll. So as a personal expert, as a personal experience of seeing people with healthspan rather than lifespan, I definitely want to be keeping up with her, with him and as I'm getting to that age. So yeah, making sure that the body's functioning and it's not running on square metal tires, that's, that's the way to go. Again. It goes, it goes quick. It'll be great to do another podcast a little bit down the track and check back in and, and give people an update. But in the meantime, again, just want to thank you for your time today. It's been really informative and for everyone listening, we'll put links straight through to the resources. So just one click away and find out more about what's going on with everything Health Span related. So thanks very much for your time. Oliver.
Oliver Ghalambor: Yeah, thank you so much.
Stuart: Perfect. Everyone, thanks for listening again and we will catch you in the next one.